Terminology as it pertains to facelift surgery can be confusing. My goal is to explain some of the differences between the procedures listed above, from my perspective, so that you can make an informed decision as to which procedures will help you accomplish your goals. Keep in mind that in facial plastic surgery, techniques chosen by surgeons are based on training, experience, results, and aesthetic judgment. A patient may have an excellent result with any of the above procedures if patient expectations are set properly and the procedure is executed with precision, skill, and artistry.
Facelift Procedure Comparison
The table below highlights the key differences between commonly performed facelift techniques.
| Procedure | Primary Area Treated | Best For | Incision Placement | Direction of Lift | Longevity |
|---|---|---|---|---|---|
| Endoscopic Midface Lift | Cheeks, lower eyelids, outer brow | Volume loss and descent of the midface | Hidden in the scalp and inside the mouth | Vertical (top-to-bottom) | Long-lasting |
| Deep Plane Facelift | Midface, jawline, neck | Significant facial and neck sagging | Around the ear and the temporal hairline | Oblique (45°) | Long-lasting |
| Uplift™ Lower Face & Neck Lift | Jawline and neck | Jowls and neck laxity | Hidden around the ear | More vertical | Long-lasting |
Deep Plane Facelift Overview
What “Deep Plane” Means in Facelift Surgery
Much attention has been given to operating in the “deep plane,” and rightly so. This refers to lifting the facial musculature and overlying tissues, generally under a layer called the superficial musculoaponeurotic system (SMAS) and often under the platysma muscle as well.
This has been extended higher in the face to dissect under the orbicularis oculi, a muscle that surrounds the eye, in an effort to approach the cheek fat pad in the midface and elevate it with its attachments to the overlying skin.
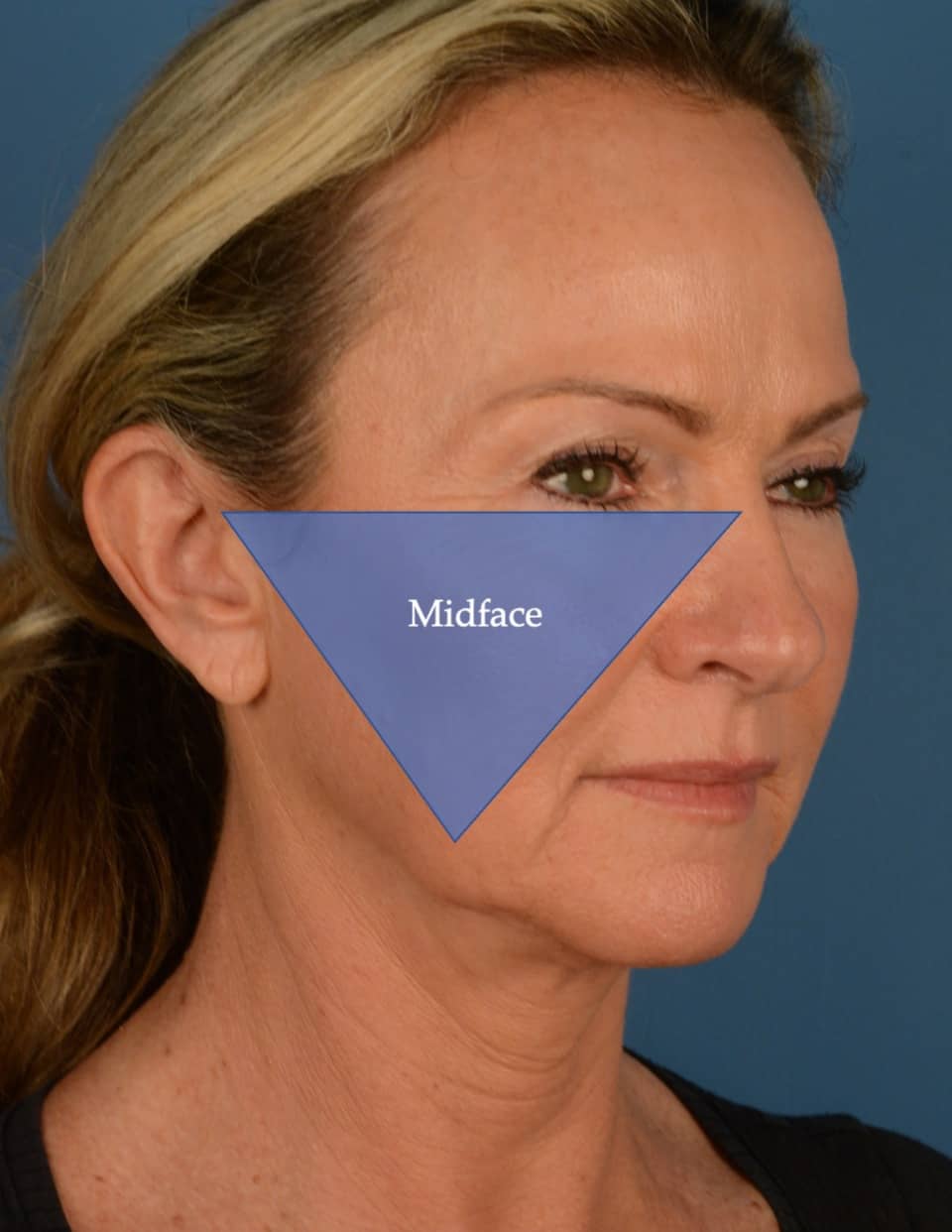
Proponents of the Deep Plane Facelift often feel that this accomplishes significant elevation of the midface (see first diagram titled “Midface Definition” – The midface is the area including the lower eyelid/cheek and extending from the ear to the nasolabial fold).
Temporal Hairline Incisions and Scar Considerations
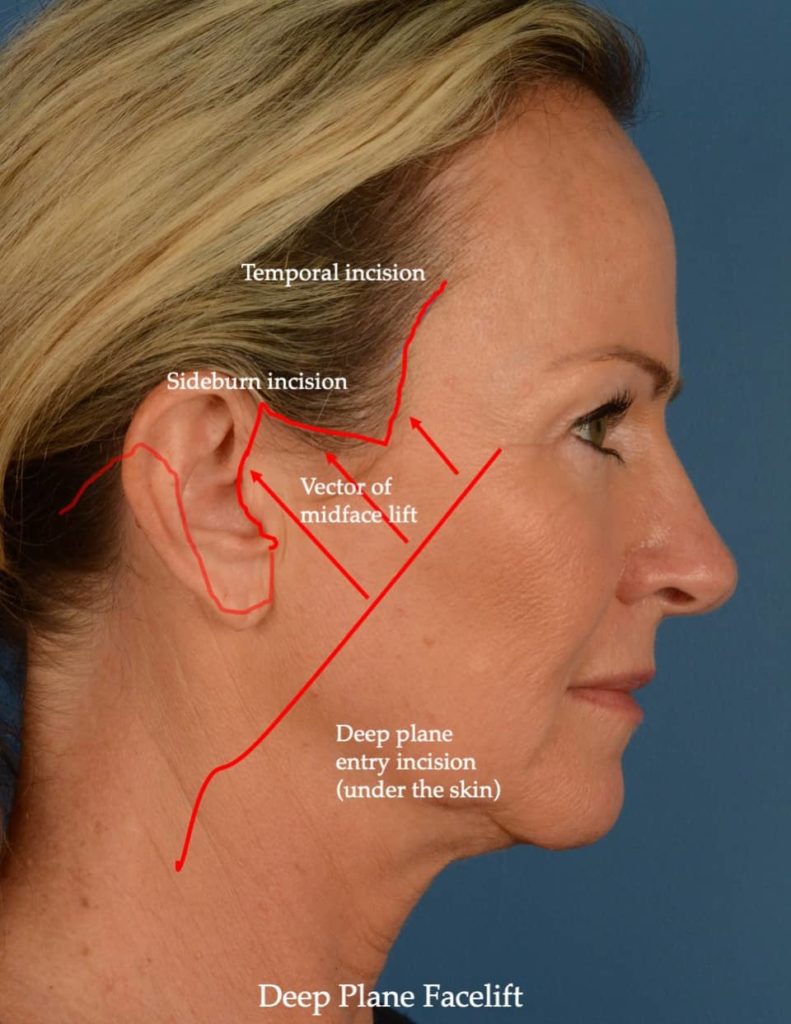
However, to significantly lift the midface with this approach, you can see in the diagram titled “Deep Plane Facelift” that the skin is recruited at a 45-degree angle by lifting the cheek.
This requires extending the incision around the temporal hairline to redrape and remove the excess skin. It is my personal preference to avoid this pre-temporal hairline scar whenever possible.
I find that when the hair is worn back and up, the scar line can be quite visible. There are some individuals that heal beautifully with this scar, but I have seen many patients who have had the Deep Plane Facelift performed by expert surgeons, and they are now obligated to wear their hair down in the temporal region to camouflage that portion of the scar or have hair transplants in front of the scars.
What Defines a True Deep Plane Facelift
One word of caution. There are many surgeons who state that they will perform a Deep Plane Facelift, but they will not actually lift the upper cheek. In this case, the incision can end below the sideburn.
However, this is not a true Deep Plane Facelift, which is meant to address the upper cheek along with the lower face and neck. Again, the only way to lift the upper cheek and redrape the skin that is elevated with a true Deep Plane Facelift is to carry the skin incision from below the sideburn up and around the front of the temporal hairline (as demonstrated in the diagram titled “Deep Plane Facelift”).
There are tremendous variations in facelift surgery and hence, the results. As an example, an Endoscopic Midface Lift can be performed in many different ways (based on extent of dissection, method of periosteal suspension, size of endoscopic incisions, use of an intraoral incision or not, etc…).
As with any plastic surgery procedure, I would recommend that you look at your surgeon’s before and after photo gallery. You should like at least 80-90% of their results, and there should be many examples of their work for you to review.

Are You Ready For A Consultation?
Schedule a consultation at Aesthetic Surgery Center in Naples, FL to receive personalized guidance from our surgical team.
Endoscopic Midface Lift Techniques
The Endoscopic Midface Lift is a procedure performed under the periosteum of the face, which means that it is performed in the deepest plane, immediately on top of the bone.
The periosteum is a fairly inelastic structure that adheres tightly to the underlying bone. When I perform an Endoscopic Midface Lift, I approach the cheek from three small entry points using an endoscope.
Hidden Incisions and Surgical Access Points
The first entry point is just above the hairline near the level of the outer eyebrow, the second is a small incision ¾ of an inch behind the temporal hairline, and the third is an incision under the upper lip, as high as you can put your tongue under your upper lip (“Sagittal Incision, Temporal Incision, Intraoral Incision” respectively in the diagram titled “Endoscopic Midface Lift”).
These are small incisions that are completely concealed (the first two by your hair and the third is inside the mouth).

Why Vertical Lift Matters
By approaching the midface from above, I feel the midface is lifted in a more vertical direction than the Deep Plane Lift. Why is this important? It is because we age in a top-to-bottom direction, not in a front-to-back direction.
Longevity of Periosteal Repositioning
In addition, after many years of performing these procedures, I believe that repositioning of the periosteum gives a longer-lasting result than lifting of the muscle layer/malar fat as performed in the Deep Plane Lift.
Periosteal repositioning and release is the basis of endoscopic forehead and brow lift surgery, which has largely replaced coronal brow lifting (ear-to-ear incisions across the scalp). This procedure has been performed for 3 decades with plenty of literature supporting the longevity of the results.
Given that the periosteum is lifted and re-adheres to the underlying bone in an Endoscopic Brow Lift procedure, the same principle applies in elevating the periosteum during an Endoscopic Midface Lift, provided a complete release of limiting facial attachments is performed.
Nasolabial Fold Improvement and Cheek Volume
What is interesting is that neither Deep Plane Facelift nor Endoscopic Midface Lift procedures reliably and consistently improve the nasolabial fold.
I have seen incredible results from both Deep Plane and Endoscopic Midface Lift techniques, in which some patients achieve improvements in the nasolabial fold. Unfortunately, nasolabial fold improvements are more uncommon than common.
Finally, the sutures used to vertically suspend the periosteum of the cheek in an Endoscopic Midface Lift cause the cheek to expand outwards slightly, giving much-needed volumization to the cheek. This helps counteract the normal cheek deflation that accompanies the aging process.
Midface Lift Before & After Photos


* Each patient is unique and individual results may vary.
The Uplift™ Lower Face and Neck Lift
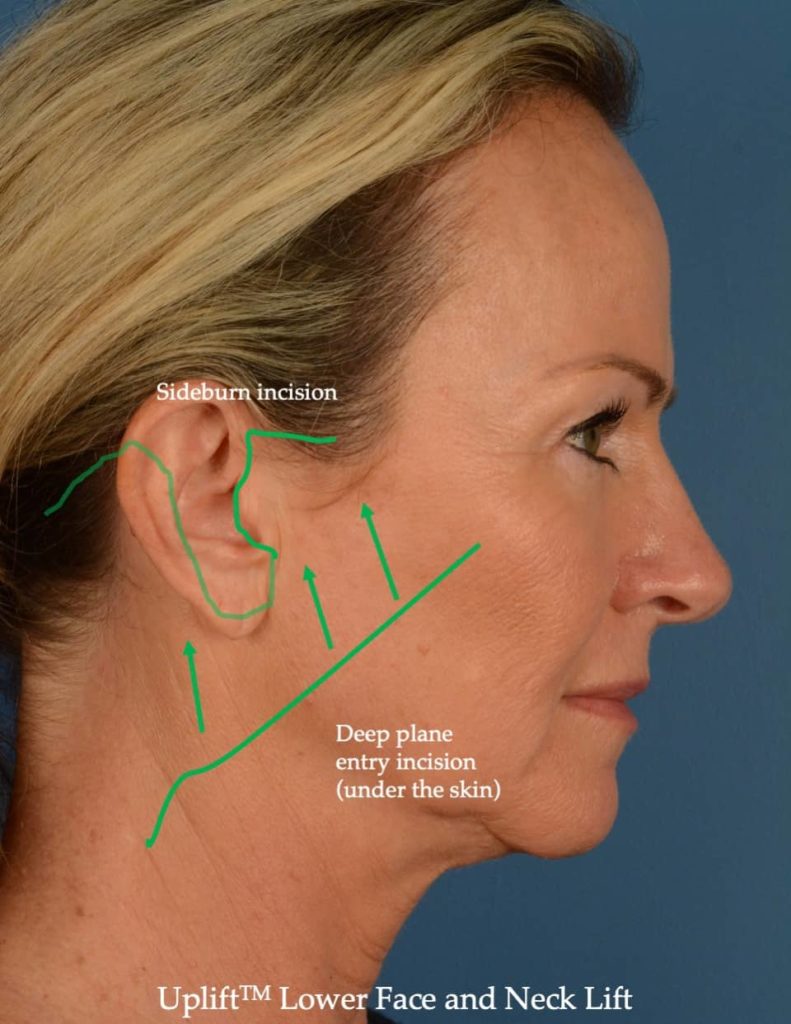
The Uplift™ Lower Face and Neck Lift is a procedure that incorporates 90% of the Deep Plane Facelift techniques but doesn’t attempt to lift the upper midface. It does lift the lower midface. Again, I do not like the temporal scar in front of the temporal hairline. The SMAS and platysmal layers are lifted in conjunction with the overlying skin.
The SMAS incision is made in a slightly more horizontal direction than the traditional Deep Plane SMAS incision, in an effort to more vertically elevate the jawline and neck (see diagram titled UpliftTM Lower Face and Neck Lift). Again, this is done to counteract the direction of aging in the most natural vector possible.
Combining Endoscopic Midface Lift with Uplift™ Lower Face and Neck Lift
Because the Endoscopic Midface Lift addresses the cheek and outer eyebrow region, I will often (but not always) perform it in conjunction with a Uplift™ Lower Face and Neck Lift.
This combination enables me to lift the cheek with the most concealed incisions possible and in a long-lasting plane of dissection, while simultaneously rejuvenating the jawline and neck.
However, it means that the surgery takes longer than a Deep Plane Facelift. To me, the trade-off in time is well worth the concealed incisions and longevity of the result.
Endoscopic Midface Lift – Advantages and Disadvantages
Advantages of the Endoscopic Midface Lift
- More vertical direction of elevation of the cheek
- No incision in front of the temporal hairline
- Increases the volume of the cheek due to imbrication (infolding of the cheek periosteum)
- Hidden incisions
- Multi-layered support (periosteum and SMAS when combined with Uplift™ )
Disadvantages of the Endoscopic Midface Lift
- Extra 1 and a half hours of surgery time
- Need for specialized endoscopic instruments
- Higher risk of infection given the intraoral incision
- Potential for increased prominence of veins around the eyes
- More prolonged cheek swelling after surgery
Schedule a Facelift Consultation Today
Choosing the right facelift technique depends on your anatomy, goals, and the surgeon’s expertise. A personalized consultation is the best way to determine which approach is most appropriate for you.
I hope this insight is helpful to you on your cosmetic surgery journey. If you would like to schedule a consultation for facial plastic surgery, please contact us at 239-594-9100.
Frequently Asked Questions About Facelift Techniques
Results are considered long-lasting. Because the periosteum is repositioned and allowed to reattach to the underlying bone, improvements often persist for many years, although the natural aging process continues.
Midface lifting can provide some improvement in nasolabial folds for certain patients, but it is not the most predictable method for eliminating them. Improvement varies depending on anatomy and the degree of volume loss.
Endoscopic midface lift incisions are small and well concealed within the hair-bearing scalp and inside the mouth, making visible scarring minimal.
A deep plane facelift lifts facial tissues beneath the SMAS and is commonly used to address the lower face and neck, while an endoscopic midface lift works at the level of the periosteum to elevate the cheek and lower eyelid area in a more vertical direction.